Section 04 of 12
When the pattern breaks: melanoma
Melanoma lacks the orderly architecture of benign lesions. Its dermoscopic features reflect disordered, asymmetric growth — and learning to recognise them is the core skill of this module.
Remember: the presence of these features moves a lesion out of the "clearly benign" category. It does not mean the lesion is melanoma — it means it deserves further evaluation.
Asymmetry of structure and colour
Benign lesions tend to be symmetric — similar structure and colour when you compare one half to the other. Melanoma disrupts this symmetry.
- Structure differs when comparing halves of the lesion
- Asymmetry in two axes is more concerning than one
- Look for asymmetric distribution of colours, network, or structures
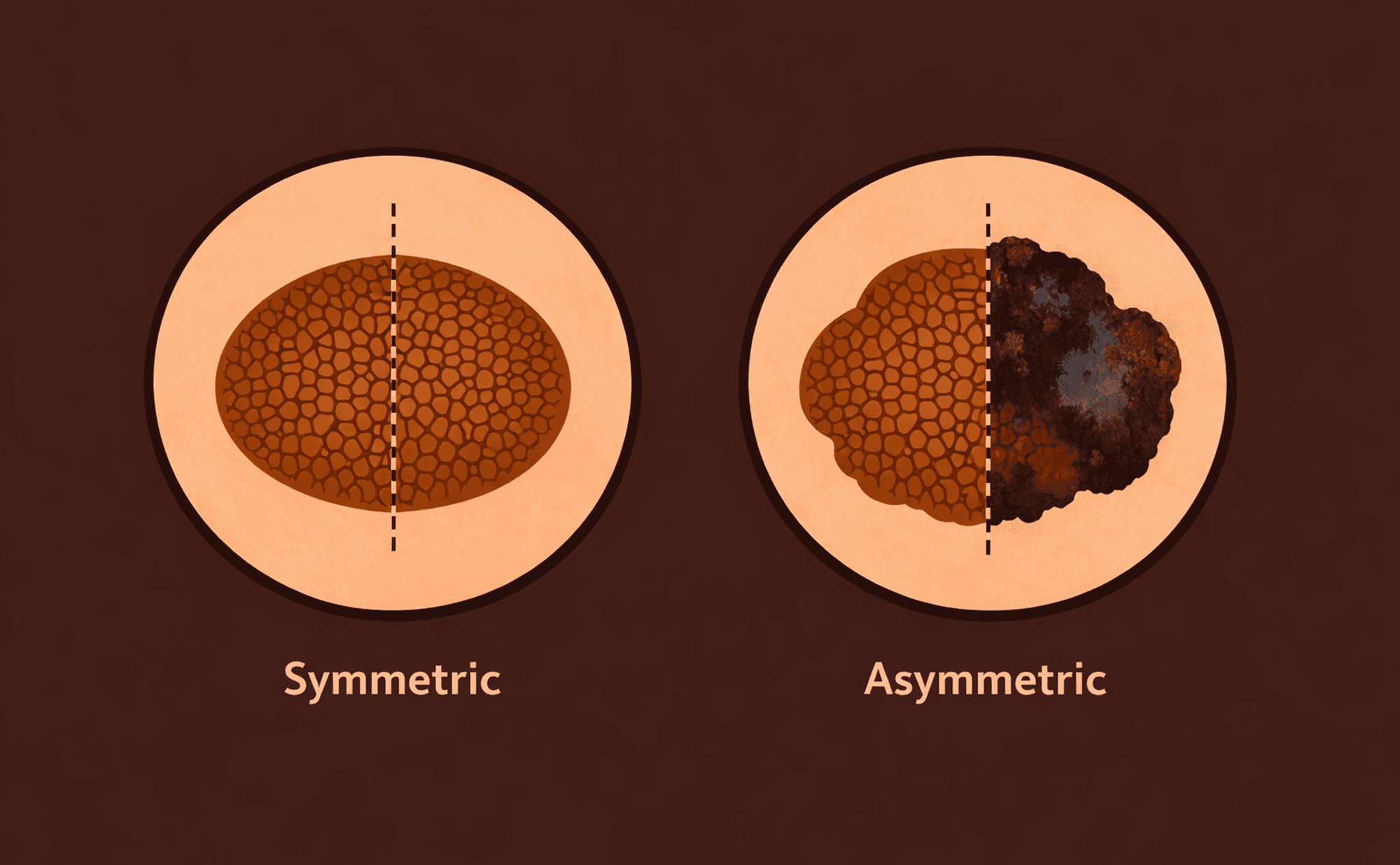
Symmetric naevus (left) versus asymmetric lesion with irregular structure and colour (right).
This is not about perfect geometric symmetry. A benign mole can be slightly oval or uneven. The question is whether the internal architecture — the patterns, colours, and structures — is distributed in an organised way.
Multiple colours
Benign lesions typically show one to two colours (shades of brown). When a lesion contains three or more colours, it suggests different biological processes happening in different areas — a hallmark of disordered growth.
The colours that matter most in dermoscopy:
| Colour | What it often indicates |
|---|---|
| Brown | Melanin in the epidermis |
| Black | Melanin at the surface (stratum corneum) |
| Blue-grey | Melanin deep in the dermis (Tyndall effect) |
| Red | Vascularity or inflammation |
| White | Fibrosis or regression |
Blue-grey colour in a melanocytic lesion always warrants attention. It indicates pigment deep in the dermis — and in the context of other concerning features, it is strongly associated with melanoma.
Atypical network
You learned the typical pigment network in Module 2 — regular spacing, uniform line thickness, gradual fading at the edges. An atypical network breaks these rules:
- Lines of unequal thickness
- Irregular holes — spaces between lines vary in size
- Abrupt termination rather than gradual fading at the edge
- Network that looks different in one part of the lesion compared to another
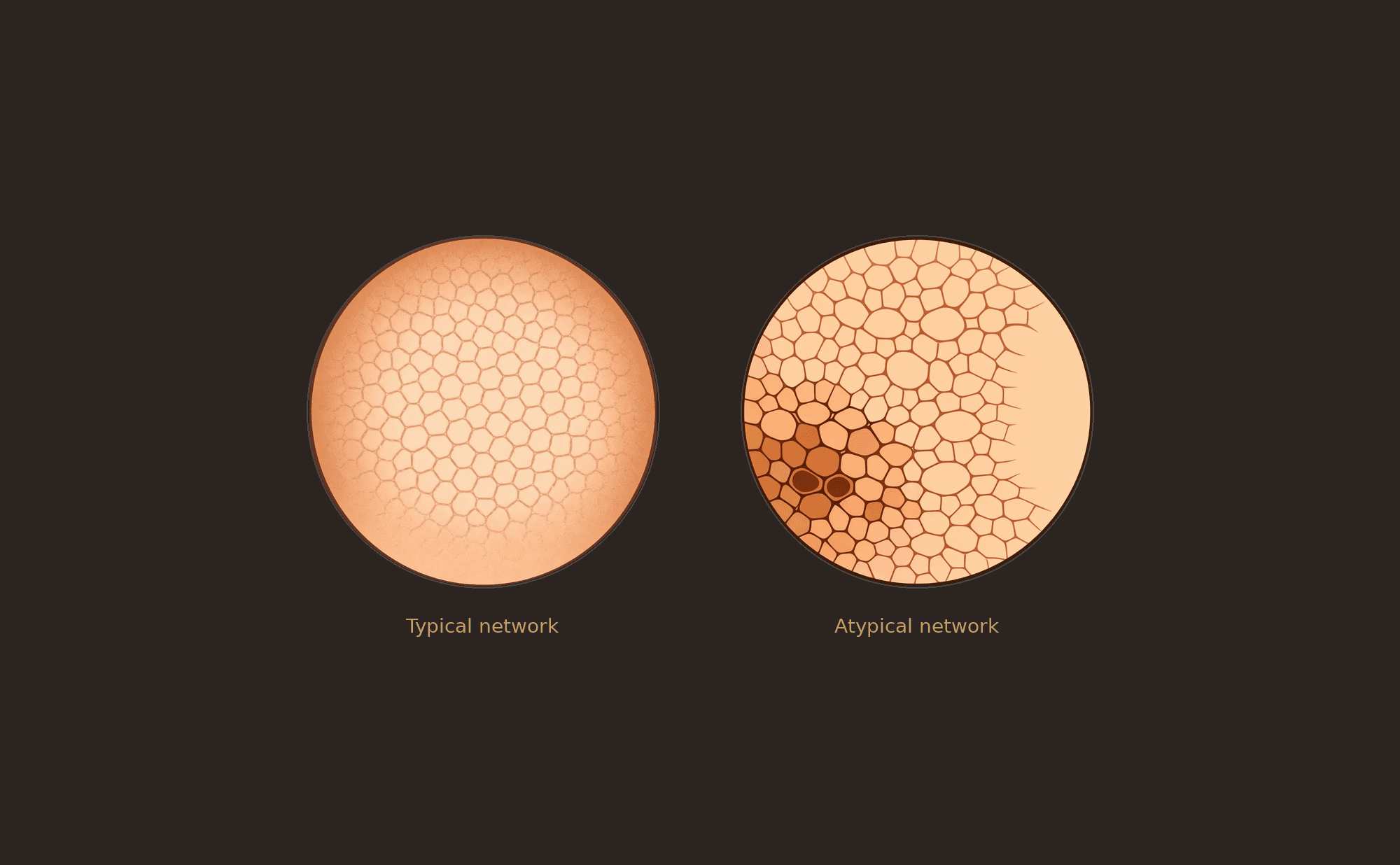
Typical network (left) versus atypical network (right) — note the irregular spacing, variable line thickness, and abrupt edge.
Think back to the fabric analogy from Module 2: a typical network is a well-made piece of fabric with even weave. An atypical network has snags, holes of different sizes, and threads that change thickness unpredictably.
Irregular dots and globules
In benign lesions, globules and dots tend to be uniform in size and evenly distributed. In melanoma:
- Variable sizes within the same lesion
- Asymmetric distribution — clustered in one area rather than spread evenly
- Different colours (brown, black, grey) within the same lesion
Irregular streaks and pseudopods
Pseudopods are finger-like projections at the lesion edge, representing radial growth. When distributed symmetrically around the entire lesion, they form a starburst pattern (seen in some benign Spitz naevi). When distributed asymmetrically — present on one side but not the other — they indicate uneven growth and raise concern.
Blue-white veil
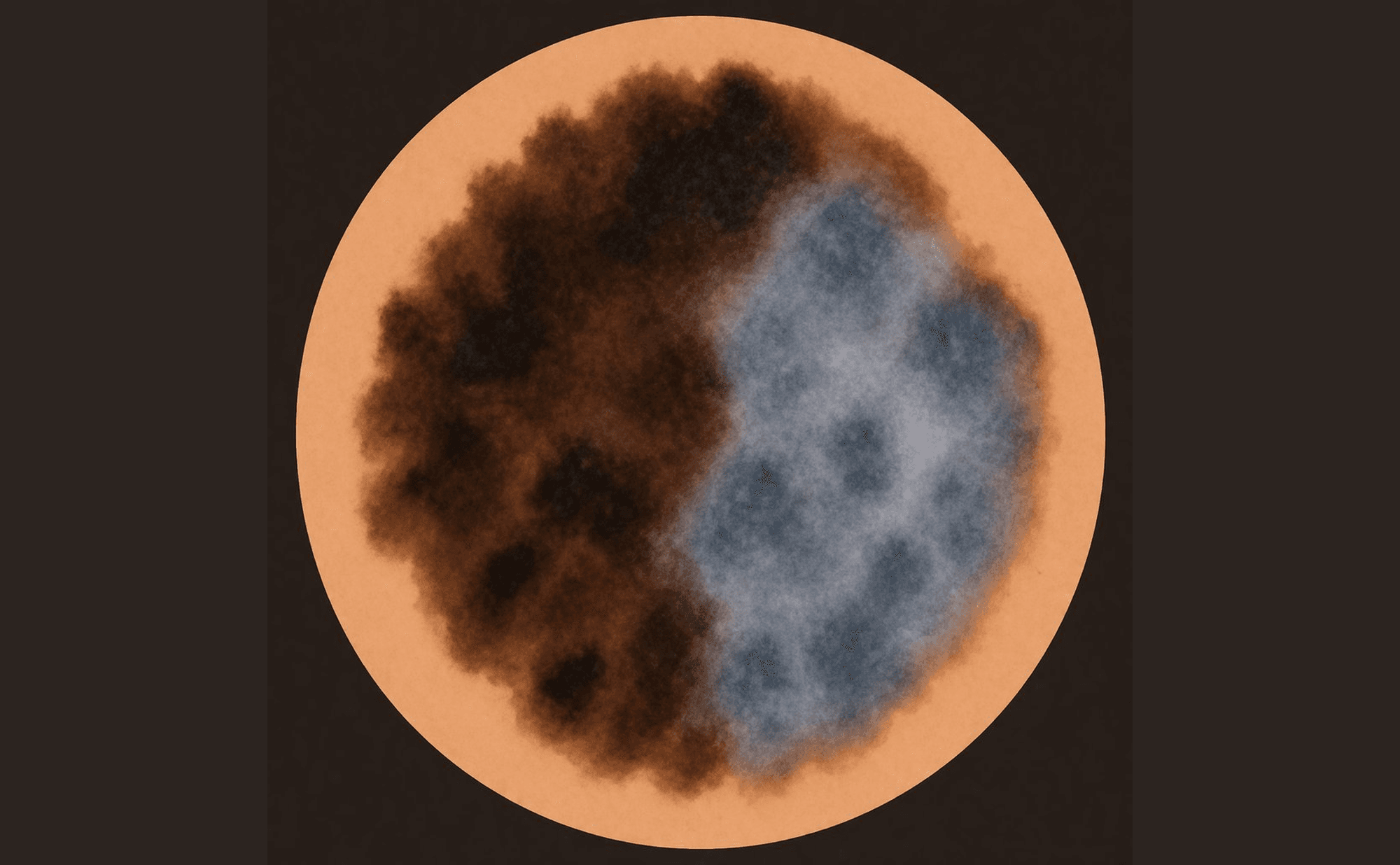
Blue-white veil — confluent blue-grey pigmentation with overlying white haze, indicating deep dermal pigment with fibrosis.
A confluent area of blue-grey pigmentation with an overlying white "ground glass" haze. This indicates pigment deep in the dermis with overlying fibrosis — and when present focally within a lesion, it is highly associated with melanoma.
Regression structures
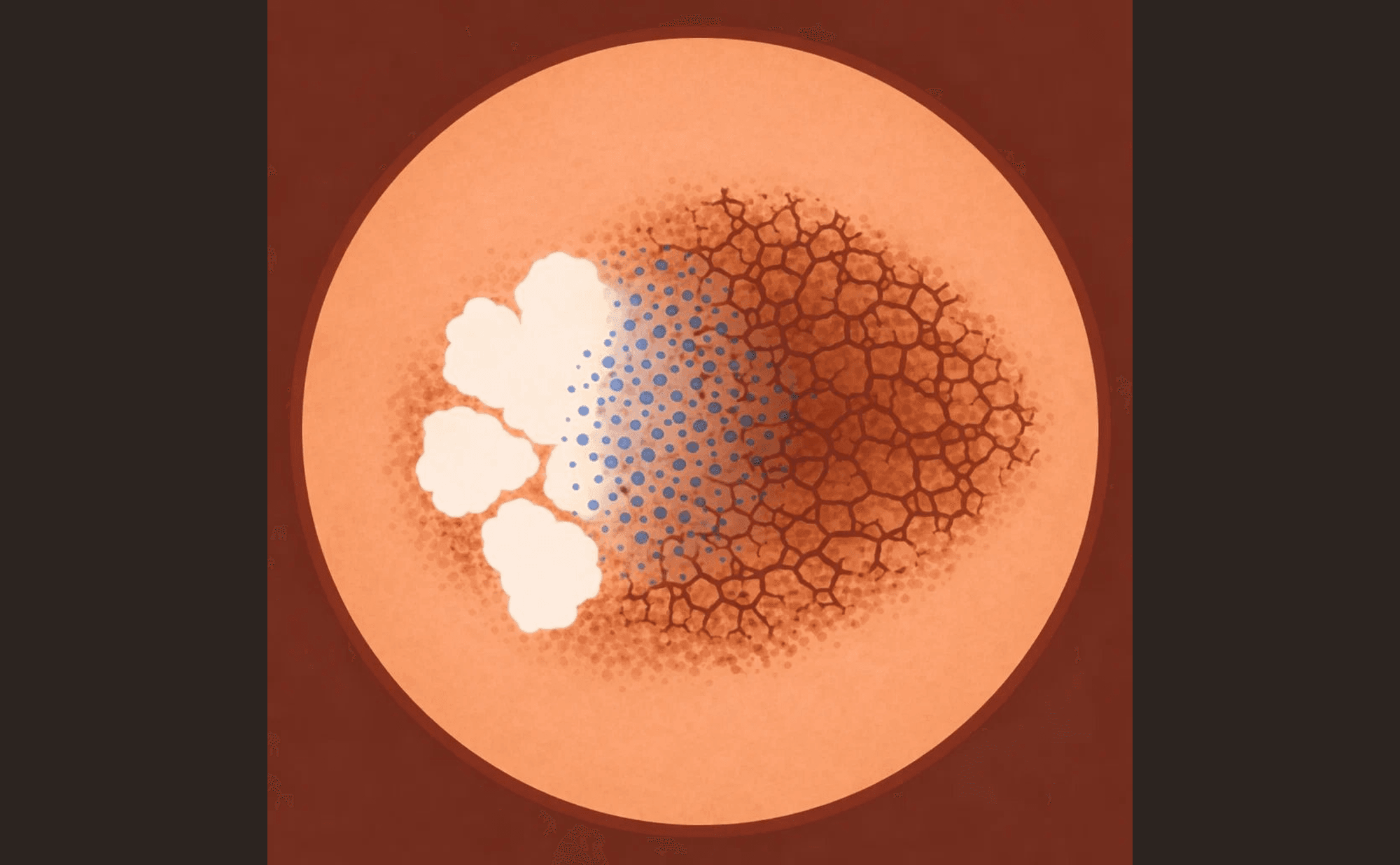
Regression structures — white scar-like areas (left), blue-grey peppering granules (centre), and disrupted residual network (right).
Areas where the lesion appears to be involuting:
- White scar-like areas — fibrosis replacing melanocytes
- Blue-grey peppering — scattered fine blue-grey granules (melanophages)
Regression indicates the immune system has attacked part of the lesion. While this sounds reassuring, regression in a melanocytic lesion can be clinically significant and warrants specialist assessment.
Atypical vessels
Vessels that do not fit the patterns you would expect for the lesion type:
- Dotted vessels irregularly distributed
- Linear irregular vessels
- Milky-red areas — pink structureless zones with vessels
Which of the following features would move a melanocytic lesion OUT of the clearly benign category? Select all that apply.