Section 05 of 10
Step 3 — Feature recognition
The question
"Are any specific high-risk features present?"
The logic
A disorganised lesion has already raised concern through its structural chaos. Step 3 now looks for specific dermoscopic features that strengthen suspicion for malignancy. The threshold is low and deliberate: the presence of any one of these seven features warrants further evaluation.
You don't need to identify what the lesion is. You need to recognise that it has features associated with malignancy and act accordingly.
The seven high-risk features
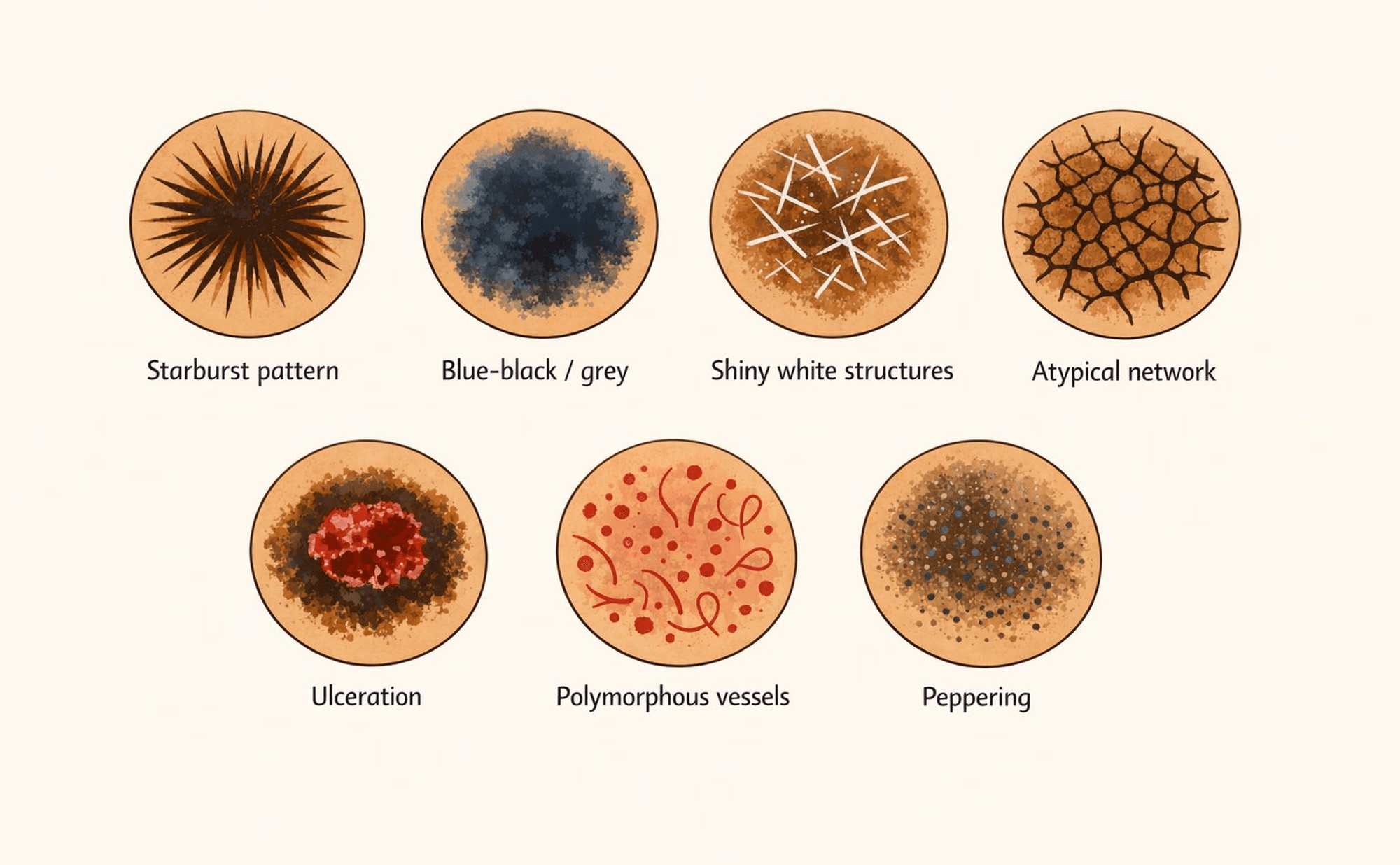
The seven high-risk features — any one of these in a disorganised lesion warrants further evaluation.
1. Starburst pattern
Streaks or pseudopods radiating from the lesion's periphery. When symmetric (projecting evenly in all directions), this pattern is associated with Spitz naevi, which still require expert evaluation. When asymmetric (projecting irregularly), the concern for melanoma increases significantly. Either way, this feature warrants further assessment.
2. Blue-black or blue-grey colour
Blue tones in dermoscopy indicate pigment deep in the dermis. Blue-white veil — a blue-grey area with a white haze overlying it — is particularly concerning. Remember the Blue-Black Rule from Module 3: any nodular lesion with blue-black colour warrants urgent evaluation regardless of other features.
3. Shiny white structures
Bright white lines, streaks, or crystalline structures visible under polarised dermoscopy. These reflect dermal fibrosis and collagen changes associated with invasive growth. Found in both melanoma and BCC.
4. Atypical network
You learned about the regular pigment network in Module 2. An atypical network has irregular line thickness, variable hole sizes, a broken or interrupted mesh pattern, and abrupt termination at the edges rather than gradual fading. It reflects disordered melanocyte growth.
5. Ulceration
Loss of the epidermis, appearing as a red structureless area, erosion, or crust. In the context of a disorganised pigmented lesion, ulceration indicates destructive growth — the tumour is breaking through the skin surface.
6. Polymorphous vessels
Multiple vessel types within the same lesion — combinations of dotted, linear, serpentine, hairpin, or irregular vessels. A single vessel type in an otherwise organised lesion is less concerning. But vascular chaos mirrors structural chaos: when you see multiple different vessel patterns in one lesion, suspicion rises.
7. Peppering (regression)
Granular blue-grey dots scattered across a portion of the lesion, sometimes called granularity. This represents regression — the immune system has destroyed part of the lesion, leaving behind melanin-laden cells in the dermis. While regression might sound like a good thing, in the context of melanoma it can obscure the original features and mask the true extent of the tumour.
The decision
If ANY feature is present — one or more high-risk features have been identified. Further evaluation is warranted through your local pathway, whether that's specialist referral, teledermatology, an urgent pathway, or senior review. The specific route varies by setting, but the conclusion is the same: this lesion needs more expert assessment.
If NO features are present — the lesion is disorganised but lacks specific high-risk features. This is a "watch closely" category. The disorganisation itself warrants vigilance. Short-interval follow-up, photographic documentation, and clear safety-netting advice are appropriate.
Which of the following are high-risk features in TADA Step 3? Select all that apply.