Section 03 of 10
Step 1 — Benign pattern recognition
The question
"Can I confidently identify this as a clearly benign lesion?"
The logic
Many lesions encountered in primary care are unequivocally benign. Recognising them immediately saves time and cognitive effort while providing appropriate reassurance. This step is the payoff for everything you learned in Modules 4, 5, and 6.
You're looking for one of three patterns:
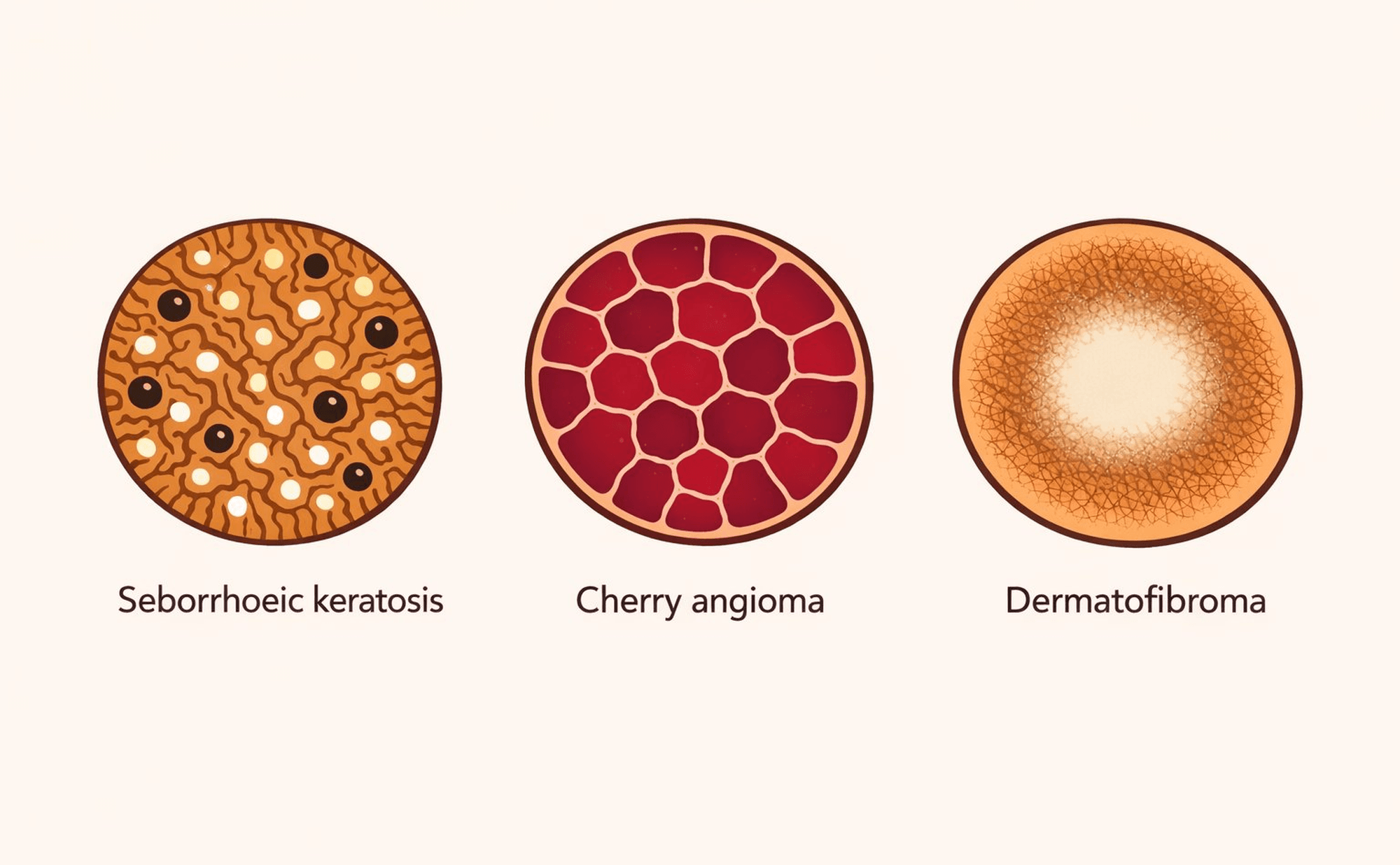
The TADA Step 1 benign trio — seborrhoeic keratosis, cherry angioma, and dermatofibroma.
Seborrhoeic keratosis (Module 4) Milia-like cysts, comedo-like openings, fissures and ridges, sharp stuck-on appearance. Remember the wobble sign.
Cherry angioma (Module 5) Red lacunae, pale septa, homogeneous red colour, sharp demarcation.
Dermatofibroma (Module 6) Central white scar-like patch, peripheral pigment network, clinical dimple sign.
The decision
If YES — the pattern is unequivocal, and you can identify the lesion with confidence — reassurance is appropriate. Document your finding. No immediate escalation is needed, though you should always apply clinical correlation.
If NO — either the pattern doesn't match, the features are ambiguous, or the lesion doesn't fit any of the three categories — proceed to Step 2.
The critical threshold
The word unequivocal is doing important work here. Only clear the lesion at Step 1 if the pattern is unmistakable. "Probably a seb K" isn't clearance — it's a sign you need Step 2. "Looks like it could be a dermatofibroma" isn't clearance either.
Think of it this way: if a colleague were watching over your shoulder and you said "that's clearly a seborrhoeic keratosis," would they agree without hesitation? If there's room for debate, the answer is no — move to Step 2.
A lesion shows comedo-like openings and a stuck-on appearance, but one area has an irregular blue-grey patch that doesn't fit the seborrhoeic keratosis pattern. What is the correct TADA Step 1 decision?