Section 03 of 09
The Classic Dermoscopic Features
Seborrhoeic keratosis has a set of hallmark dermoscopic features. When multiple features are present together, identification is highly reliable. Think of these as the "fingerprint" of the lesion — distinctive, recognisable, and consistent.
Milia-like cysts
Small, round, white or yellow-white structures scattered across the lesion surface. They look like tiny pearls embedded in the skin — bright, well-defined, and clearly distinct from the surrounding pigmented background.
These are milia-like cysts, and they represent small collections of keratin trapped within the epidermis. Under the dermatoscope, they catch the light and appear as bright dots against the darker background of the lesion.
They are one of the most recognisable features in all of dermoscopy. When you see multiple bright white dots scattered across a well-defined pigmented lesion, seborrhoeic keratosis should be your first thought.
Comedo-like openings
Dark, round or oval plugged openings on the lesion surface. They look like blackheads — small, dark puncta set into the surface of the lesion.
These comedo-like openings are keratin-filled invaginations — essentially, small plugged openings in the skin surface. They are the visual opposite of milia-like cysts: where milia-like cysts are bright against a dark background, comedo-like openings are dark against a lighter background.
Together, milia-like cysts and comedo-like openings form the classic duo of seborrhoeic keratosis. Seeing both in the same lesion is strongly diagnostic.
Fissures and ridges
The surface of many seborrhoeic keratoses shows a pattern of grooves and raised lines that creates a distinctive texture. The analogy most dermoscopists use is a brain-like or cerebriform pattern — the surface folds and furrows much like the surface of the cerebral cortex.
These fissures and ridges reflect the bumpy, papillomatous surface architecture of the lesion. They are easiest to see in thicker, more raised seborrhoeic keratoses and may be subtle or absent in flat variants.
Sharp demarcation
Seborrhoeic keratoses typically have a clearly defined edge — a crisp boundary where the lesion ends and normal skin begins. This sharp demarcation reflects the well-circumscribed nature of the growth. The lesion does not fade gradually into the surrounding skin the way a benign naevus might.
In some cases, the border has a distinctive scalloped, concave quality known as a moth-eaten border — as if small bites have been taken out of the edge.
Putting the features together
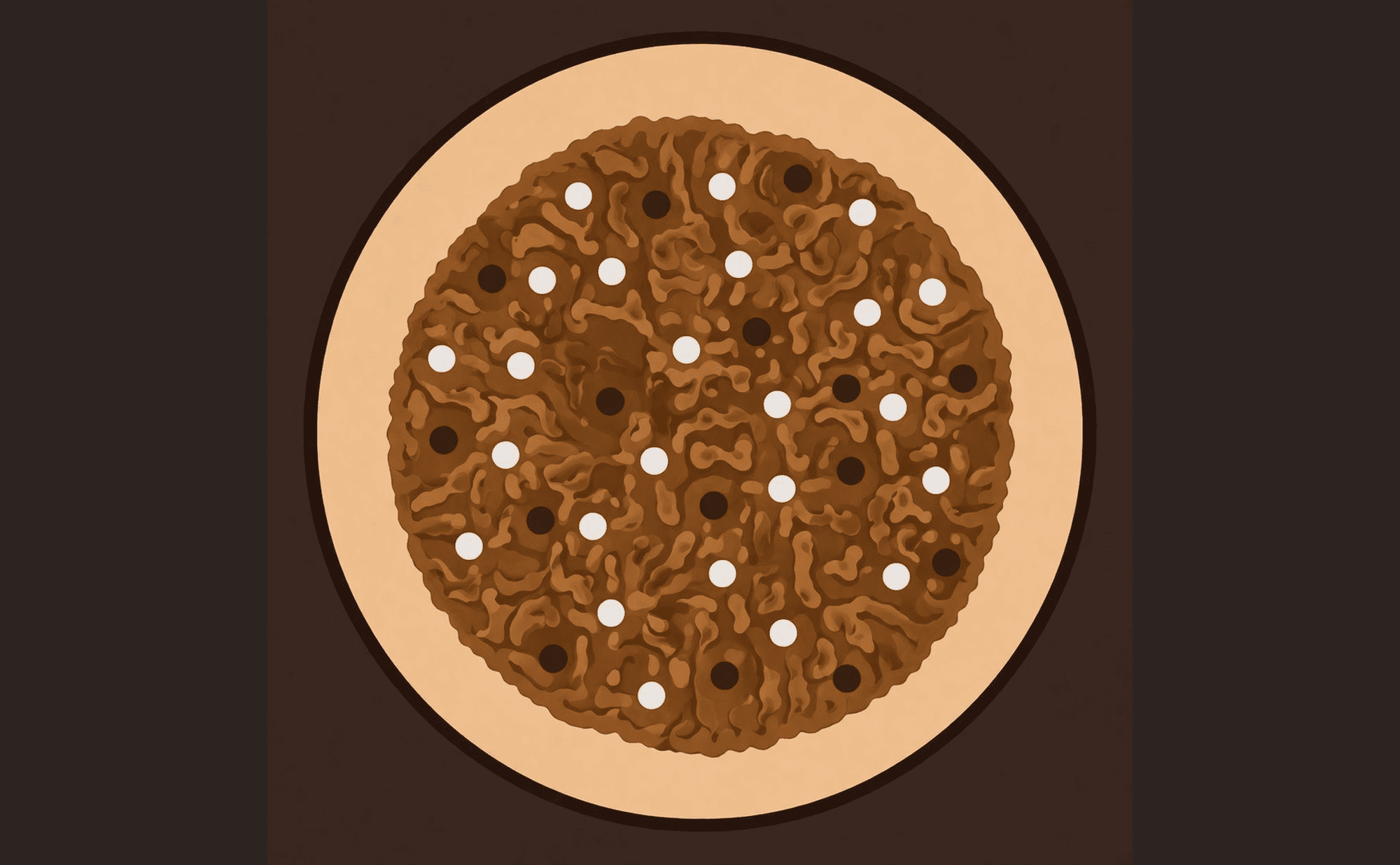
Classic SK: milia-like cysts (white dots), comedo-like openings (dark dots), cerebriform pattern, and sharp border
No single feature is diagnostic on its own. Milia-like cysts can occasionally appear in other lesions. Comedo-like openings alone are not conclusive. But when you see multiple classic features in the same lesion — especially the combination of milia-like cysts, comedo-like openings, and a cerebriform surface — the pattern becomes distinctive and reliable.
The classic triad: milia-like cysts + comedo-like openings + fissures and ridges. When all three are present in a well-demarcated lesion, you can identify seborrhoeic keratosis with high confidence.
Which combination of dermoscopic features is most characteristic of seborrhoeic keratosis?